Introduction of
microbiology
The term of
microbiology compose three word.
1- Micro mean – so small can't seen by neked eye.
2- Bio mean – living.
3- Logy mean – science.
So micro
biology is defined as the study of microbes or living microorganisms of microscopical
size.
Microorganisms
were first seen about 1675 by Layven hook. He found many microorganisms in
material such as water, saliva and intestinal content of healthy subject.
The term
(microbe) was introduced by Louis paster (1857 – 1860) whose demonstration that
fermentation was caused by the bacterial and yeast growth.
The term
microbe was used by Sedillat in 1878 but now is replaced by microorganism.
Robert Koch
1877 described methods for microscopic examination of bacteria in dried fixed
films stained dyes and in 1881 devised the simple method for isolating pure
culture of bacteria by plating out mixed of single bacteria grow in separate
colonies.
Prokaryotes
and Eukaryotes
All
microorganisms that are capable of self multiplication can be differentiated by
their cell type into one of two groups.
1.
Prokaryotic 2. Eukaryotic
Prokaryotic
|
Eukaryotes
|
|
Cell structure
|
Very simple
|
Complex
|
Nuclear membrane
|
Absent
|
Present
|
Genetic material
|
Lies in cytoplasm
|
Contained in nuclear membrane
|
Mitochondria
|
Absent
|
Present
|
Enzymes
|
Contain simple enzyme
|
Contain complex enzyme
|
Type of multiplication
|
By binary fission
|
By mitosis
|
Examples
|
This group in include bacteria rikettesia, chiomydia
and mycoplasma
|
This group includes protozoa and fungi, moulds&
algae
|
The algae,
protozoa, moulds and fungi their cell have the some general type of structure
and organization, they are described as eukaryotic.
Viruses
1.
Viruses are the smallest intracellular microorganism that containing
only one kind of nucleic acid (DNA or RNA) as their genome.
2.
Viruses can pass through bacteria stopping filter. All species are
strictly parasites.
3.
Can grow only in living cells, non can grow on an inanimate nutrient
media.
4. Viruses are distinguished from
other many bacteria by having an entirely different method of growth and
reproduction.
The Bacteria
are a group of single-cell microorganisms with procaryotic cellular
configuration. The genetic material (DNA) of procaryotic cells is not contained
within a nucleus, which is the definitive characteristic of eukaryotic cells,
such as those that make up plants and animals.
Bacterial cells
structure
Structurally, a procaryotic cell (Figure 1 below) has
three architectural regions: appendages (attachments to the cell
surface) in the form of flagella and pili (or fimbriae); a cell
envelope consisting of a capsule, cell wall and plasma
membrane; and a cytoplasmic region that contains the cell genome (DNA)
and ribosomes and various sorts of inclusions.

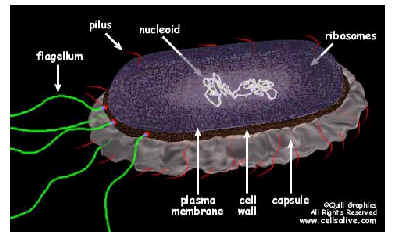

Table 2. Summary: Characteristics of typical
bacterial cell structures
|
||
Structure
|
Function(s)
|
Predominant
chemical composition
|
| Flagella | Swimming movement | Protein |
Pili
|
||
Sex
pilus
|
Mediates
DNA transfer during conjugation
|
Protein
|
Common
pili or fimbriae
|
Attachment
to surfaces; protection
|
Protein
against phagotrophic engulfment
|
Capsules
(includes "slime layers" and
glycocalyx)
|
Attachment
to surfaces; protection against phagocytic engulfment, occasionally killing
or digestion; reserve of nutrients or protection against desiccation
|
Usually
polysaccharide; possible polypeptide
|
Cell
wall
|
||
Gram-positive
bacteria
|
Prevents
osmotic lysis of cell protoplast and confers rigidity and shape on cell
|
Peptidoglycan
(murein) complexed with teichoic acids
|
Gram-negative
bacteria
|
Peptidoglycan
prevents osmotic lysis and confers rigidity and shape; outer membrane is
permeability barrier; associated LPS and proteins have various functions
|
Peptidoglycan
(murein) surrounded by phospholipid protein-lipopolysaccharide "outer
membrane"
|
Plasma
membrane
|
Permeability
barrier; transport of solutes; energy generation; location of numerous enzyme
systems
|
Phospholipid
and protein
|
Ribosomes
|
Sites
of translation (protein synthesis)
|
RNA
and protein
|
Inclusions
|
Often
reserves of nutrients; additional specialized functions
|
Highly
variable; carbohydrate, lipid, protein or inorganic
|
Chromosome
|
Genetic
material of cell
|
DNA
|
Plasmid
|
Extrachromosomal
genetic material
|
DNA
|
The cell wall
The layers
of the cell envelope lying between the cytoplasmic membrane and capsule.
The cell
wall provides protection and imports shape to the cell.
The cell
wall of gram positive (G+ve) bacteria differ in its structure and composition
form that of gram negative (G-ve)
In the Gram-positive
Bacteria (those that retain the purple crystal violet dye when subjected to
the Gram-staining procedure) the cell wall is thick, consisting of several
layers of peptidoglycan as well as teichoic acids.
In the Gram
negative Bacteria (which do not retain the crystal violet) the cell wall is
relatively thin and is composed of a single layer of peptidoglycan (no teichoic
acid) surrounded by a membranous structure called the outer membrane.
The outer membrane of Gram-negative bacteria invariably contains a unique
component, lipopolysaccharide (LPS or endotoxin), which is
toxic to animals.
The
Plasma Membrane or Cytoplasmic
membrane (Cell membrane or plasma membrane).Its main function is a selective
permeability barrier that regulates the passage of substances into and out
of the cell. It is barrier between interior and exterior of the bacterial cell.
The Cytoplasm
The cytoplasm of most bacteria contain DNA,
ribosomes RNA and storage granule.
Storage
granule
Temporarily
hold excess metabolites storage granule known as volutine and lipid granules
(metachromatic granules).
DNA, double – stranded circular molecule.
Plasmid is extra chromosomal circular and smaller then DNA.
Plasmids carry genes involved in antibiotic resistance called.
Ribosomes: composed 2 subunit. One with a sedimentation
coefficient of 50 Sved berg units (50s) and other 30s = 70s.
RNA: The function of RNA is translation of Genetic code
tram DNA for protein synthesis.
The
capsule or glycocolyx.
Many bacteria secret around themselves polysaccharide
substance, often referred to as a slime layer. This may become sufficiently
thick to form a definite capsule around the organism.
1. protects the cell from
phagocytosis.
2. adherence of bacterium to surface
of the cells (tissue).
3. Virulence factor
Flagella
-
Arrangement basis for classification
-
Monotrichous; 1 flagella
-
Lophotrichous (polar
flagella); tuft at one end
-
Amphitrichous; both ends
-
Peritrichous; all around
bacteria
Flagella:
present in many bacteria, it is
responsible for motility.
-
Peritrichous flagella: many
flagella distributed over the bacterial surface.
-
Monotrichous flagella:
bacteria have a single flagellum.
-
Polar flagella: the bacteria
have small bundle of flagella located atone end.
Pili
or Fimbriae:
1. Protein fibers that cover the
entire surface of G-ve bacteria
2. Ploy a major in bacterial
adherence to the cell surface.
3. Sex pili involved in bacterial
conjugation (and gene transfer).
Classification
of microorganisms
The
majority of microorganisms maybe classified in the following biological groups.
1. Algae. 2. Protozoa. 3. Mould. 4.
Fungi 5. Bacteria. 6. Spirochaetes. 7. Mycoplasmas. 8. Chlamydiaceae. 9.
Rickettsieae. 10. Viruses
Morphological
classification of bacteria
Morphologically
bacteria car resemble.
Cocci (singular: coccus)
Coccobacilli (singular:
coccobacillus)
Rods
(bacilli) (singular: rod, bacillus)
Vibrios (singular: vibrio)
Spirilla (singular: spirillum)
Spirochetes (singular:
spirochete)

Staphylococcus aureus
Staphylococcus: are cluster
forming Gram positive cocci.
The
main species of medical importance is: staphylococcus aureus. Other species may
also cause disease include S.epidermidis and S.saprophyicus.
Habitat: widely
distributed in the environment. They form part of the normal microbial flora of
the skin, upper respiratory tract and intestinal tract. S. aureus is carried in
the nose of 40% or more of healthy people.
Pathogenicity
S. aureus causes boils, styes, pustules, impetigo,
infections of wounds (cross-infections), ulcers and burns, osteomyelitis,
mastitis, septicaemia, meningitis, pneumonia and pleural empyema.
Also, toxic food-poisoning (rapid onset, no fever),
toxic shock syndrome and toxic skin exfoliation. S. aureus is carried in
the nose and on the skin of many healthy people. It is easily spread in
hospitals, particularly on surgical wards.
Extracellular enzymes and toxins produced by strains
of S. aureus that contribute to its invasiveness and pathogenicity
● Coagulase: Clots plasma, interferes with
phagocytosis, facilitates spread in the tissues.
● Haemolysins: Lyze red cells.
● Leukocidin: Kills leucocytes.
● Fibrinolysin: Digests fibrin.
● Lipase: Breaks down fat.
● Hyaluronidase: Facilitates spread in tissues
by destroying hyaluronic acid (component of connective tissue).
● Protein A: Antiphagocytic (prevents
complement activa-tion).
● Enterotoxins (heat stable): Cause
food-poisoning (particularly vomiting).
● Toxic shock syndrome toxin-1: Shock, rash,
desquamation of skin.
● Epidermolytic toxins A and B: Generalized
peeling of the skin.
● Chemotaxis inhibitory protein: Inhibits
migration and activation of neutrophils.
LABORATORY FEATURES
Specimens: Pus and swabs
from infected sites, sputum, cerebrospinal fluid, blood for culture. Faeces,
vomit and the remains of food when foodpoisoning is suspected.
Morphology
Staphylococci are Gram positive cocci of uniform size,
occurring characteristically in groups but also singly and in pairs. They are non-motile
and non capsulate.
Culture
Staphylococci grow well aerobically and in a carbon
dioxide enriched atmosphere. Most strains also grow anaerobically, but less
well. Temperature range for growth is 10–42 oC, with an optimum of
35–37oC .
Blood agar, chocolate (heated blood) agar: S. aureus produces yellow (golden
yellow) to cream or occasionally white 1–2 mm in diameter colonies. Pigment is
less pronounced in young colonies. Some strains are betahaemolytic when grown aerobically. Colonies
are slightly raised and easily emulsified.
MacConkey agar: Smaller (0.1–0.5
mm) colonies. Most strains are lactose fermenting.
On
Mannitol salt agar:selective and
differential media for S.aureus isolation from faecal specimens when
investigating staphylococcal food-poisoning and nasal carrier screening. S.aureus
ferment manitol and the colonies surrounded by yellow zones due to acid
production.
S. aureus ferments
mannitol and is able to grow on agar containing 70–100 g/l sodium chloride.
Mannitol salt agar containing 75g/l sodium chloride (plus 4 mg/l methicillin) is
recommended, particularly for isolating MRSA strains.
Biochemical tests: S. aureus is:
● Coagulase positive.
● DNA-ase positive.
● Catalase positive.
latex agglutination test kits are available to identify
S. aureus based on the detection of clumping factor and, or, protein A
Pastorex Staph Plus test
It detects all strains of S. aureus, including
up to 95% MRSA strains (reagent contains antibodies to the capsular
polysaccharides found in MRSA as well as fibrinogen and protein A).
Dryspot Staphytect Plus
It detects up to 97% of S. aureus strains,
including most MRSA. Colonies of S. aureus are emulsified in saline and mixed
with the dry reagent. Agglutination of the blue latex particles indicates a
positive test.
Commercially available test kits to confirm MRSA
Test kits have become available to detect penicillin
binding protein 2 (PBP2) for the rapid detection of MRSA. An example of a PBP2
latex agglutination test is Mastalex MRSA. The test has been shown to be
97% specific and sensitive for the
detection of MRSA. PBP2-based tests are expensive.
Antimicrobial susceptibility
Antibiotics with activity against S. aureus include:
Penicillins* Vancomycin, Macrolides, Cephalosporins and Fusidic acid *Most
strains of S. aureus (particularly hospital strains) are resistant to
penicillin due to the production of plasmid-coded beta-lactamase.
MRSA (methicillin resistant S. aureus): These strains
are resistant to methicillin and related penicillins and are particularly difficult
to treat because they are also resistant to most other common antibiotics. Vancomycin
is often needed to treat MRSA infections.
Other pathogenic Staphylococcus species
_ Staphylococcus saprophyticus: Causes
urinary tract infections in sexually active women.
_ Staphylococcus epidermidis: May cause
endocarditis and bacteraemia following infection of cannulae, indwelling
catheters, shunts or other appliances positioned in the body. Infections are
difficult to treat due to the resistance of S. epidermidis to many
antimicrobials.
Microscopically: S. saprophyticus and S.
epidermidis resemble S. aureus.
Culturally the colonies of S. epidermidis are
white and usually non-haemolytic. The colonies of S. saprophyticus may
be white or yellow. They are non-haemolytic. Growth may not occur on MacConkey
agar. S. saprophyticus and S. epidermidis are coagulase negative.
Biochemical reactions that differentiate
S. epidermidis and S. saprophyticus from S. aureus
Test
S. aureus S. epidermidis S. saprophyticus
Coagulase + –– –
DNA-ase + +Weak –
Mannitol* + - +
Trehalose* + - +
Sucrose* + + +
Novobiocin (5µg)S S R
Notes: *Fermentation tests: __Sugar fermented
with acid production (sugar tablet tests are available from Rosco Diagnostics) S
_ Susceptible, R _ Resistant
Streptococcus pyogenes
Classification of streptococci and enterococci
These organisms are broadly classified by their
haemolytic activity on blood agar (alpha, beta, non-haemolytic) and
by Lancefield group antigens in their cell wall (envelope). Streptococci,
formerly classified as Group D streptococci, are now included in the genus Enterococcus
e.g. S. faecalis has been reclassified E. faecalis.
Pathogenicity
S. pyogenes (Lancefield Group A) causes sore throat (tonsillitis,
pharyngitis), peritonsillar abscess (quinsy), scarlet fever, otitis media,
cellulitis, impetigo, necrotizing fasciitis, rysipelas, puerperal sepsis,
septicaemia, and occasionally toxic shock syndrome. Also immune mediated
post-streptococcal rheumatic fever (following throat infections) and glomerulonephritis
(after skin or throat infections).
Note: S. pyogenes can be found as a
commensal in the upper respiratory tract, particularly of children.
Extracellular enzymes and toxins produced by strains
of S. pyogenes that contribute to its invasiveness and pathogenicity
●Streptolysins (toxins that haemolyze red cells):
– Streptolysin S that is active aerobically (beta-haemolysis
on blood agar). It is non-antigenic. Streptolysin O that haemolyzes red cells
under anaerobic conditions, e.g. sub-surface agar stabs. It is antigenic, stimulating
the production of antistreptolysin O antibody (ASO), see later text.
● Streptokinase, a protease that lyzes fibrin.
● Hyaluronidase: Facilitates spread in the
tissues by destroying hyaluronic acid.
● Leukocidin: Destroys leucocytes.
● Lipoteichoic acid: Facilitates adherence to
pharyngeal epithelial cells.
● M-proteins (antigens): Anti-phagocytic
virulence factors.
● NADase (nicotinamide adenine
dinucleotidase): Kills leukocytes. Antibody formed after infection.
● DNA-ases (deoxyribonuclease) A, B, C, D
that break down DNA and stimulate an antibody response, particularly against
DNA-ase B. Anti-DNA-ase B tests are available.
● Erythrogenic toxin: Responsible for the
rash seen in scarlet fever and is also associated with streptococcal toxic
shock syndrome..
LABORATORY FEATURES
Specimens: Throat swab (avoiding saliva contamination)
or swabs of pus and serous fluid depending on the site of infection, and blood
for culture.
Culture media should be inoculated as soon as
possible or a swab placed in a tube of silica gel.
Testing for ASO antibody in serum is helpful in
diagnosing rheumatic fever.
Morphology
Streptococci are Gram positive cocci, occurring
characteristically in short chains, but also in pairs and singly. Long chains
are formed in fluid cultures. The organisms are non-motile. Some strains are
capsulated.
Culture
Blood agar: S. pyogenes produces beta-
haemolytic colonies(the colonies are surrounded by a zone of complete
haemolysis). Colonies are usually small (0.5–1 mm), colourless, dry, shiny or
mucoid. Haemolysis is more marked under anaerobic conditions as seen in
colonies growing below the agar surface (following stabs made in the culture
medium).
Choice of blood
To isolate beta-haemolytic streptococci, use
sheep blood (1st choice), horse, rabbit or goat blood to prepare blood agar
plates. Do not use human blood because this may contain unwanted substances
such as citrate (e.g. donor blood), antibiotics, or antibodies such as ASO or anti-M
protein that could interfere with the growth or haemolytic activity of S.
pyogenes.
Sensitivity to bacitracin
Adding a bacitracin disc (0.04 or 0.05 IU, not
higher), to a plate of blood agar or preferably a selective medium, is a useful
method of screening for S. pyogenes. Most strains are sensitive to
bacitracin, but it is not possible to rely completely on sensitivity to bacitracin
to identify S. pyogenes. Other non-Group A beta-haemolytic
streptococci (e.g. Groups B, C and G) may occasionally also show sensitivity to
bacitracin. Serological grouping is required.
Note: S. pyogenes is always sensitive
to benzylpenicillin and therefore placing a 1 µg disc of the antibiotic on a primary
culture plate (well area) can also help topresumptively identify S. pyogenes.
Crystal violet (1 in 50 000) blood agar: This is a useful
inexpensive selective medium for isolating S. pyogenes from patients
with impetigo where S. aureus may be present with S. pyogenes.
Crystal violet will inhibit the growth of S. aureus. Alternatively, use
a 30 µg neomycin disc on the heavy part of the inoculum.
MacConkey agar: S. pyogenes does not grow on
this medium.
Biochemical tests: S. pyogenes is:
● Catalase negative (staphylococci are positive)
● PYR positive*
*PYR (pyrrolidonyl) test: This detects
pyrrolidonyl peptidase enzyme activity. Besides S. pyogenes, Enterococcus
species and occasionally streptococci belonging to groups C and G are also
PYR positive. The test can be rapidly and simply performed using PYR
impregnated strips.
S. pyogenes belongs to
Lancefield Group A can be grouped (identified) using specific Group A antiserum
to identify the A antigen extracted from the cell wall of the bacteria (coagglutination or latex) to Lancefield group betahaemolytic
streptococci.
Positive group A
test:Indicates
that the organism is S. pyogenes (particularly when bacitracin sensitive and
PYR positive) but possession of A antigen is not species specific. Very
occasionally other beta haemolytic streptococci group as A.
Direct detection of antigen A from throat swab
extracts:
Several tests can be used to detect antigen A directly extracted from throat
swabs without the need to culture the specimen, Most of the rapid direct tests
are immunochromatographic (IC) enzyme immunoassays (with built-in control) or
latex agglutination techniques.
ASO antibody tests
Measurement of ASO antibody in serum ASO
(anti-streptolysin O) antibody is formed in response to infection with S.
pyogenes and other streptococci that produce streptolysin 0 (some Group C
and G strains).
Rapid, simple to perform latex agglutination to screen
for and measure semi-quantitatively raised levels of ASO antibody in serum.
Measurement of ASO antibody titre is important in
the investigation of post-streptococcal diseases, particularly rheumatic fever.
In rheumatic fever there is a rise in ASO antibody titre in 80–85% of patients.
The rise begins early in the course of the disease with highest levels being
reached soon after onset of the disease. In the second week, the level begins
to fall. Rheumatic fever is a serious post-streptococcal complication because
it can lead in later life to chronic valvular disease of the heart.
Measurement of DNA-ase B antibody
Most increases in DNA-ase B (deoxyribonuclease B) antibody
titres occur in response to Group A streptococcal infection. The rise in DNA-ase
B antibody usually occurs later than the rise in ASO antibody. Measurement of
anti-DNA-ase B is of value when investigating acute glomerulonephritis
following a streptococcal skin infection (rather than a streptococcal sore
throat). This is because the ASO antibody titre is not usually raised following
streptococcal skin infections whereas there is a rise in titre of anti-DNA-ase
B.
Antimicrobial susceptibility
susceptible to penicillin. Erythromycin is usually
used to treat patients hypersensitive to penicillin but resistance to
erythromycin (and also to tetracyclines) is being increasingly reported.
Streptococcus agalactiae
Pathogenicity
Streptococcus agalactiae (Lancefield Group
B) causes septic abortion and puerperal or gynaecological sepsis, and occasionally
urinary tract infection. S. agalactiae forms part of the normal microbial
flora of the female genital tract. Occasionally it causes neonatal septicaemia
and meningitis.
In cattle S. agalactiae is a common cause
of bovine mastitis. Human strains are distinct from animal strains.
LABORATORY FEATURES
Specimens: Include cerebrospinal fluid, ear swab, and
blood for culture from neonates. High vaginal swab is required from women with
suspected sepsis.
Morphology
Group B streptococci are Gram positive cocci,
occurring characteristically in short chains but also in pairs and singly. The
organisms are non-motile. Most strains are capsulated.
Culture
Blood agar: Most
strains produce grey mucoid colonies about 2 mm in diameter, surrounded by a
small zone of betahaemolysis (clear area with decolorization of
haemoglobin). About 5% of strains are nonhaemolytic. Placing discs of
penicillin and gentamicin on the plate can help to identify these strains
(penicillin sensitive, gentamicin resistant).
MacConkey agar: Most
strains grow on this medium. Neomycin blood agar: A useful selective medium for isolating S. agalactiae from
urogenital specimens.
Orange pigment: Produced
by S. agalactiae when cultured on serum starch agar anaerobically.
Lancefield grouping
S. agalactiae belongs to Lancefield Group B. Serological
identification of the organism can be made by detecting B antigen using Group B
antiserum reagent. The technique is similar to that described for grouping Streptococcus
Group A.
CAMP (Christie, Atkins, Munch, Peterson) test
This test requires the use of a beta-lysin
producing strain of S. aureus to detect the CAMP factor, i.e.
extracellular diffusible protein produced by S. agalactiae. This protein
interacts with the staphylococcal beta-lysin on sheep (or ox) blood agar
producing enhanced haemolysis.
Bile aesculin stope: S. agalactiae does not
hydrolyse aesculin. It is able to grow on bile agar. Group A Streptococcus pyogenes
gives a variable aesculin hydrolysis reaction and does not grow on bile
agar. Group D streptococci hydrolyse aesculin and can grow on bile agar.
Hippurate hydrolysis test
S. agalactiae hydrolyzes hippurate
Direct detection of Group B streptococcal antigen in
c.s.f.
When Group B streptococcal meningitis is suspected, a
rapid diagnosis can be made by detecting Group B streptococcal antigen directly
in c.s.f., serum or urine using a latex or coagglutination slide test. They are
particularly useful if antibiotic treatment has been started and it is not
possible to isolate S. agalactiae culturally.

Fig . CAMP reaction of Streptococcus agalactiae (Group
B).
Antimicrobial susceptibility
S. agalactiae has the same susceptibility
profile as S. pyogenes.
Streptococcus pneumoniae
Pathogenicity
S. pneumoniae causes lobar pneumonia,
bronchitis, meningitis, bacteraemia, otitis media, sinusitis and
conjunctivitis.
Serotypes: Over 80 capsular serotypes of S.
pneumoniae have been identified. Less than 15 serotypes are responsible for most
infections.
LABORATORY FEATURES
Specimens: Depending on the site of infection,
specimens include sputum, exudate, blood for culture, and cerebrospinal fluid.
Morphology
S. pneumoniae is a Gram positive elongated
(lanceolate) diplococcus. It also forms short chains, particularly following
culture. Pneumococci are nonmotile and capsulated (non-capsulated following culture).
In Gram stained smears from specimens, the capsule can often be detected as an
unstained empty area around the diplococcus.
Culture
Blood agar: Following overnight incubation.
S. pneumoniae forms translucent or mucoid colonies, 1–2 mm in diameter.
In young cultures the colonies are raised but later become flattened with raised
edges, giving them a ringed appearance (‘draughtsmen’). Strains of some
serotypes (e.g. serotype 3) produce large mucoid colonies. Pneumococci show alpha-haemolysis.
Note: When cultured anaerobically on blood agar,
some strains of S. pneumoniae show betahaemolysis.
Viridans streptococci: These
organisms which may be found in sputum are also alphahaemolytic and require differentiation
from S. pneumoniae
Optochin sensitivity
Pneumococci are sensitive to optochin
(ethylhydrocupreine hydrochloride). Placing a disc (5µg) on a primary sputum
culture and culturing the plate aerobically (not in CO2 ) can help
to provide a rapid presumptive identification of S. pneumoniae. If the zone
of inhibition is less than 10 mm (6 mm disc) the colonies should be tested for
bile solubility.
Chocolate and lyzed blood agar: S. pneumoniae grows well on
chocolate (heated blood) agar and lyzed blood agar. Growth is enhanced when
incubated in a carbon dioxide enriched atmosphere (candle jar).
Biochemical tests: S. pneumoniae is
● Catalase negative ● Sensitive to optochin ● Bile
soluble
*Bile solubility test
There are several ways of testing pneumococci for
bile solubility. Some workers, however, prefer to test suspect alpha-haemolytic
colonies directly on a culture plate by touching a colony with a loopful of 2% sodium
deoxycholate reagent (pH.7.0), incubating the plate at 35–37 ؛C
for 30 minutes, and examining for lysis (disappearance of the colony,
indicating S. pneumoniae).
Direct detection of pneumococcal antigen in body
fluid
Rapid latex and coagglutination tests are available
to detect capsular pneumococcal antigen in c.s.f., pleural fluid, serum and
urine.
Antimicrobial susceptibility
Antibiotics with activity against pneumococci
include penicillin, erythromycin, and co-trimoxazole. Penicillin-resistant strains
are becoming an increasing. When testing for susceptibility to penicillin it is
best to use a disc containing 1 µg of oxacillin. A zone size less than 20 mm
indicates reduced susceptibility. Isolates should also be tested for susceptibility
to tetracycline, erythromycin and chloramphenicol.
Viridans streptococci
Although often alpha-haemolytic on blood
agar, the viridans group of streptococci can also be nonhaemolytic and
occasionally beta-haemolytic. They form part of the normal microbial
flora of the upper respiratory tract (particularly oropharynx) and
gastrointestinal tract. They may therefore be found with S. pneumoniae in sputum (as commensals). A
few species are pathogenic (e.g. S. mutans, S. sanguis, S.
mitior) causing endocarditis, bacteraemia, and dental caries. The following
are the main features which differentiate S. pneumoniae from viridans
streptococci:

The S. anginosus group (formerly S.
milleri group) is associated with deep abscesses in various sites in the
body (abdomen, chest, brain) often in association with other bacteria.
Anaerobic streptococci and
cocci
Most of the pathogenic Gram positive anaerobic streptococci
and cocci belong to the genus Peptostreptococcus.
Anaerobic streptococci and cocci can be found as commensals
on the skin and in the mouth, vagina and gastrointestinal tract. They can cause
septicaemia, puerperal sepsis, and bone and joint infections. They are often
isolated together with other anaerobes such as Bacteroides fragilis, from
abscesses and deep infected wounds and ulcers. Many strains are proteolytic and
gas (H2S)-producing producing unpleasant smell.
Anaerobic streptococci and cocci can be cultured in thioglycollate
broth. On subculture to blood agar, the colonies are very small, shiny, and
nonhaemolytic. Incubation for up to 72 hours is often required to produce
visible growth. Microscopically: They
appear as Gram positive cocci in chains, groups, or singly, variable in size,
and catalase negative. Anaerobic cocci are usually susceptible to penicillin,
and all are susceptible to metronidazole 5 µg disc).
Enterococcus species
Pathogenicity
E. faecalis (formerly classified Streptococcus.
faecalis) is the main pathogen in the genus Enterococcus, causing
about 95% of enterococcal infections including infections of the urinary tract,
biliary tract, ulcers (e.g. bed sores), wounds (particularly abdominal) and
occasionally. Endocarditis or meningitis. It is a normal commensal of the
vagina and intestinal tract. A minority of infections are caused by E.faecium.
LABORATORY FEATURES
Morphology
Enterococcus species are Gram positive cocci,
occurring in pairs or short chains. They are non-capsulate and the majority are
non-motile.
Culture
Enterococci are aerobic organisms capable of growing
over a wide temperature range, 10–45 OC.
Blood agar: Enterococci are mainly
nonhaemolytic but some strains show alpha or beta-haemolysis.
MacConkey and CLED agar: E. faecalis ferments
lactose, producing small dark-red colonies on MacConkey agar and small yellow
colonies on CLED (cysteine lactose electrolyte-deficient) agar.
Enterococcus species are also able to grow in the
presence of 6.5% sodium chloride and 40% bile. Withstand 60 OC for
30 minutes and can grow at 45 OC. When grown on media containing aesculin,
enterococci hydrolyze the aesculin, producing black colonies.
Biochemical tests: Enterococcus species:
● Ferment lactose (also mannitol and other sugars).
● Hydrolyze aesculin.
● Reduce litmus milk.
Lancefield group: Enterococci possess
Lancefield Group D antigen (as also some streptococci). E. faecalis,
however, is usually identified culturally and biochemically.
Antimicrobial susceptibility: Most are
susceptible to ampicillin and resistant to cephalosporins. Resistance to
penicillin.
|
Table
show: Biochemical reaction of
Streptococci
|
|||||
|
CAMP
test
|
Litmus
milk reduction
|
Sensitivity
to optichin& bile salt
|
Bacitracn
sensitivity
|
Catalase
|
Species
|
|
-
|
-
|
-
|
+
|
-
|
S-pyogenes(A)
|
|
+
|
-
|
-
|
-
|
-
|
S-aglactiae
(B)
|
|
-
|
+
|
-
|
-
|
-
|
Entrococci(D)
|
|
-
|
-
|
-
|
-
|
-
|
Viridans
strept
|
|
-
|
-
|
+
|
-
|
-
|
S-pneumoniae
|
Bacillus anthracis
Pathogenicity
B. anthracis causes anthrax which is mainly a disease
of sheep, cattle, goats and other herbivores with humans becoming infected only
after coming into contact with infected animals or their skins.
Anthrax in animals
Animals
become infected by ingesting B. anthracis when feeding. Pastureland that
has become contaminated with spores from excreted bacilli or from the bodies of
dead animals (highly infectious) can remain a source of infection for many
years, e.g. 50–60 y.
Sources of anthrax in humans
Human infections (zoonoses) can occur from handling
infected animals or coming into contact with skins containing anthrax spores, when
using skins as clothing, water-carrying containers, or sleeping mats. Other
sources of infection include animal hair, bones, and the bedding of infected
animals. Less commonly, infection is caused by eating infected meat.
Depending on the source and site of infection, B.
anthracis can cause:
_ Cutaneous anthrax (commonest form):
Bacilli enter damaged skin, producing a blister (‘malignant pustule’) which
usually ulcerates and eventually forms a dry black scab surrounded by oedema. Fatal
septicaemia, toxaemia, and meningoencephalitis may develop, especially in non-immune
persons. Ocular anthrax may also occur.
_ Pulmonary anthrax: Caused by inhaling large
numbers of B. anthracis spores (‘woolsorters’ disease). Infections are
usually fatal.
_ Enteric anthrax: A severe form of
gastroenteritis with fever, abdominal pain and bloody diarrhoea, due to
ingesting infected meat. Septicaemia often develops.
_ Meningoencephalitis: Usually as a
complication of septicaemia and occasionally as primary anthrax meningoencephalitis.
Virulence factors
B. anthracis produces a polypeptide capsule which is antiphagocytic
and a toxin which affects the central nervous system leading to respiratory
distress, shock, cardiac collapse and death.
LABORATORY FEATURES
Specimens: Include fluid aspirated from cutaneous lesions
and when indicated, sputum, cerebrospinal fluid, and blood for culture.
Caution: B. anthracis is a high risk
infectious pathogen, therefore handle specimens and infected material with care.
Morphology
B. anthracis is a large, 5–8X1.5 µm, Gram positive (or
Gram variable) non-motile bacillus, often appearing joined end to end in
chains.
In smears from specimens: Bacilli are
capsulated. The capsular material often appears irregular and fragmented. When stained
using Loeffler’s polychrome (McFadyean) methylene blue the bacilli stain blue
and the capsular material stains purple-pink. Giesma stain can also be used
when MacFadyean methylene blue is not available.
In smears from aerobic cultures: Bacilli are
non-capsulated but contain oval spores (same diameter as the bacilli), giving
the organisms a beaded appearance. They occur in chains.
Culture
B. anthracis grows
aerobically and anaerobically (facultative anaerobe). The temperature range for
growth is 12–45 OC with an optimum of 35–37OC. Spore
formation is best between the range 25–30 OC.
Blood agar: B.
anthracis produces large 2–5 mm in diameter, grey-white, irregular colonies with
wavy edges. The colonies are nonhaemolytic or only slightly haemolytic. Saprophytic
Bacillus species are markedly haemolytic.
Broth cultures: They
are not usually turbid, but they often show a thick skin (pellicle) and a sediment.
Gelatin stab culture: The
organism slowly liquefies the gelatin along and out from the line of
inoculation. The treelike pattern formed by the liquefaction lines is characteristic
of B.anthracis, but the reaction is slow and in practice anthrax bacilli
are usually identified microscopically by their morphological appearance.
Antimicrobial susceptibility
Antibiotics with activity against B.
anthracis include penicillin, tetracycline, streptomycin, and
co-trimoxazole. Workers at risk of infection should be vaccinated.
Bacillus cereus
B. cereus toxin
causes food-poisoning, usually in rice or other cereals that have been cooked
and then stored in warm temperatures. B. cereus unlike B. anthracis is
motile, non-capsulate, and produces haemolytic colonies on blood agar. Non-lactose
fermenting, producing pale colonies on MacConkey agar. On egg-yolk agar, B.
cereus gives a strong lecithinase reaction. It rapidly liquefies gelatin
stabs.
Mannitol egg-yolk phenol-red polymyxin
agar (MYPA) is recommended as a selective medium for the isolation of B.
cereus from faeces, vomit, or food. After overnight incubation at 35–37 OC,
large 3–7 mm flat, dry grey-white colonies surrounded by an area of white
precipitate are produced. B. cereus produces beta-lactamase and is resistant to
penicillin
and cephalosporins. Antimicrobials
with activity against B.cereus include gentamicin, erythromycin, vancomycin
and clindamycin.
Corynebacterium diphtheriae
Pathogenicity
C. diphtheriae causes:
_Nasal, nasopharyngeal and tonsillar
diphtheria, especially in young children. Often there is marked oedema of the
neck. Infection is by inhaling respiratory droplets.
Exotoxin
Virulent strains of C. diphtheriae produce
a powerful exotoxin that is absorbed through the damaged mucous membrane into
the blood circulation. If not neutralized by antitoxin, the toxin can cause
toxaemia with fatal cardiac and neural complications.
At the site of infection there is an
acute inflammatory response which leads to the formation of a grey-yellow membrane
which becomes necrotic at a later stage. If this membrane extends downwards to
the larynx it can blockthe passage of air and cause death from asphyxia.
_ Cutaneous (skin) diphtheria
which usually develops when C. diphtheriae infects open wounds.
C. diphtheriae biovars. There
are four biovars (biotypes): gravis, intermedius, mitis,
and belfanti. These names were used to describe the severity of disease.
In the investigation of diphtheria, it is not necessary to differentiate these biovars.
Note: Commensal
diphtheroids form part of the normal microbial flora of the upper respiratory
tract and skin.
LABORATORY FEATURES
The role of the laboratory is to confirm the
clinical diagnosis.
Specimens:
Include throat, and, or nasopharyngealswabs to confirm a diagnosis of throat
diphtheria, and a skin swab if cutaneous diphtheria is suspected.
Morphology
C. diphtheriae is
Gram positive(stains unevenly and weakly). It is markedly pleomorphic. Long,
thin, and curved forms can be seen and also short rods and rods enlarged at one
end (clubshaped). They often appear in clusters, joined at angles like Chinese
letters.
Commensal diphtheroids: These
are strongly Gram positive and stain uniformly. They are usually short and show
little variation in size and form.
Volutin granules. In Albert stained smears, particularly from
Loeffler serum or Dorset egg cultures, C. diphtheriae often appears
beaded due to the presence of darkstaining granules in the rods. These granules,
known as volutin or metachromatic granules, in toluidine blue stained smears, the
organisms stain pale blue and the granules dark red-purple.
C. diphtheriae is
non-capsulate, non-motile, and does not form spores.
Culture
C. diphtheriae is
an aerobe and facultative anaerobe. Temperature range for growth is 20–40 OC
with an optimum of 35–37 OC. Loeffler
serum medium and Dorset eggmedium: C.
diphtheriae grows rapidly on these media, producing significant growth in 4–6
hours.
Note: It
is not advisable to use either Dorset egg or Loeffler serum medium as a primary
medium for isolating C. diphtheriae because commensal diphtheroids may overgrow
the diphtheria bacteria.
Tellurite blood agar: Used
as a primary medium for isolating C. diphtheria from throat and
nasopharyngeal swabs.
C. diphtheriae reduces
tellurite and produces grey or grey-black colonies measuring 0.5–2 mm in
diameter. Single colonies are generally darker or blacker than those massed
together.
Some strains are raised and cone-shaped
(especially mitis), others are raised with striated margins and grey
centres (especially gravis), and others are small with black centres and
clear margins (especially intermedius). Strains can be haemolytic,
slightly haemolytic, or non-haemolytic. Mitis strains are beta-haemolytic.
Commensal diphtheroid colonies are grey,
non-haemolytic, and measure 0.1–0.8 mm in diameter. Separate colonies are
generally paler than those massed together. Some staphylococci and streptococci
also produce black colonies on tellurite blood agar.
Tinsdale medium: After
24–28 h incubation, C. diphtheriae colonies are grey-black, raised, and
surrounded by a dark brown area as shown in. The brown colour is due to the
hydrogen sulphide produced from the cystine interacting with the tellurite. Occasionally commensal diphtheroids and other respiratory
tract commensals may grow on Tinsdale’s medium but the colonies are not surrounded
by a brown halo like those of C. diphtheriae. Proteus species
produce large colonies with a blackening in the medium.
Tinsdale medium in addition to tellurite
also contains cystine which makes it more differential for C. diphtheriae (browning
is produced in the medium).
Biochemical tests: C.
diphtheriae:
● Catalase and nitrate positive.
● Oxidase negative.
● Urease negative.
● Ferments glucose and maltose with acid
production. A few strains of gravis and mitis biovars ferment
sucrose.
● C. diphtheriae gravis ferments
starch with acid production.
Rapid carbohydrate utilization test to identify C.
diphtheriae and other Corynebacterium species
ليست هناك تعليقات:
إرسال تعليق